Disc Injury
Does improvement towards a normal Cervical Sagittal configuration aid in the management of Lumbosacral Radiculopathy
PUBLISHED: 2015, Journal of Chiropractic Medicine 14 (2). Pub Med: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4523573/
AUTHORS: Moustafa IM, Diab AA, Harrison DE.
Proceedings of the 13th World Federation of Chiropractic Biennial Congress / ECU Convention, Athens, Greece, May 13-16, 2015. Paper #184 Mediterranean Region Award Winning Paper.
INITIAL CONCLUSIONS: Improvement of normal cervical sagittal configuration aids in the management and rehabilitation of patients with lumbosacral disc disruption and radiculopathy.
Correcting Lower Back Disc Injuries
Case History: Chronic Lower Back Pain, Disc Herniation and Prolapse
This is not a testimonial. This is a Case Study of a real patient who attended the Practice.
Mr. B. is a 47 year old male factory worker that attended the Practice with acute debilitating lower back pain and disability. His diagnosis was that of lower back disc injuries (L3, L4 and L5). He was suffering chronic spinal pains, mid back and lower back pain with associated myofascial (muscle) weakness in the lumbopelvic region.

Congratulations To Ilja
It is not just about the pain you are in; it is the impact it has on your life.
One of our fantastic patients, Ilja placed first in a recent golf tournament. Braving some terrible conditions he won first place in +3 par competition. Still a fair bit of work to do but happy with how he played.
The smiling chap above is a long way from the severely stressed patient that first attended the Practice with chronic neck pain and disability.
It is not just about the pain you are in; it is the impact it has on your life. You become the limitations of your injury as opposed to living a life you want to live.
Failed Back Surgery Syndrome
Case History: How We Help If You’ve Had Back Surgery.
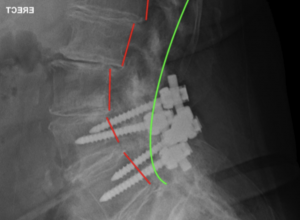
Mrs. A is a 78 year old patient who attended the practice with chronic lower back pains and general disability. She had FOUR (4) lower back surgeries. The patient was due for surgery number five but decided on a different, more conservative path.
Looking at the X-ray of the lower back, you will note she had multiple fusions with metal rods. The metal fixations were ‘power drilled’ into the spine with four large self tapping screws. The screws hold two plates across the base of the spine.

Correcting ‘Australian Posture’ – Chronic Back Pain
Case History: Chronic Lower Back Pain, Forward Head Carriage and ‘Australian Posture’
Mr. M. is a 44 year old male sales and office worker who attended the Practice. Yes a real patient, real person.
He was suffering with chronic lower back pain (CLBP). He had been enduring spinal pain for 25 years and things were getting progressively worse.
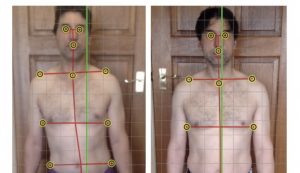
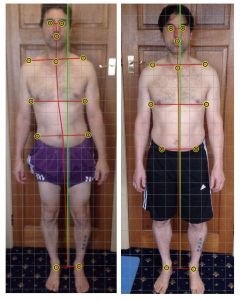
In terms of postural distortion; Mr. M. had what we affectionally call an ‘Australian Posture’. Australian Posture is something we commonly see in Practice and is a driver of many lower back and neck conditions.
Australian Posture is the forward translation of the torso and head forward of the vertical green axis line, in the manner you see below. Not only does this create tremendous pressure on the lower back, but also the neck and shoulders.
Case History: Patient with Lower Back Disc Injury
Mr. B. is a 47 year old male factory worker that attended the Practice with acute debilitating lower back pain and disability. He was suffering chronic spinal pains, mid back and lower back pain with associated myofascial (muscle) weakness in the lumbopelvic region.
He could not work, walk, sit or sleep without significant sharp and stabbing pains into the lower back, aching and weakness in to the legs. Prior to attending the Clinic the patient had a series of cortisone injections into the spine with little effect. He was using Lyrica and Panadene.
The patient had been referred to a surgeon in preparation of the lower back disc removal and fusion. The patient was informed the surgery would cost approximately $100,000.00. He attended the Practice for a second opinion.
This is the result of his care:
Introducing The Musculoskeletal Profile
Many patients really struggle with neck pain, back pain, headaches, arthritis, stress and chronic pains.
And of those patients, it is bewildering that many have years of treatment with varying practitioners, spending thousands of dollars – and NEVER having these key nutrients tested.
It is highly unlikely you will ever achieve a great outcome in the care if these key values are not right.
Now optimal is the key here.
Near enough is not good enough.
If you are paying north of $60 a visit to a therapist or practitioner you need to have the key nutrients at the optimal level to get the best out of your care. You need to get this right.
If you are using natural medicines or health supplements you need to know if they are working and you are taking the correct amount.
Further more being in a ‘normal’ range is quite different than being in an optimal range to encourage the body to heal.